Chronic cough in dogs is a common presenting complaint in small animal practice. Often, clients want immediate relief for their dog, such as antitussive medication; however, antitussives are not indicated until specific diseases have been ruled out or appropriately managed. This is because coughing can be an appropriate physiologic response (initiated by cough receptors in the larynx, trachea, and bronchi) to many different triggers (e.g., environmental irritants such as smoke or other insults such as inflammation, excessive mucus accumulation, aspirated food or water, and airway foreign bodies). Treating these underlying problems takes priority over mere cough suppression; however, determining these underlying causes of cough can be challenging.
In general, chronic cough in dogs can occur secondary to cardiac disease, respiratory disease, or both. Cardiac causes include left-sided congestive heart failure and advanced heartworm disease. Respiratory causes are numerous and can be inflammatory (e.g., chronic bronchitis, eosinophilic bronchopneumopathy [EBP]), infectious (i.e., bacterial, fungal, protozoal, viral, parasitic), degenerative (e.g., airway collapse, bronchiectasis), trauma (e.g., inhaled foreign body or gases), aspiration pneumonitis (e.g., secondary to dysphagia or laryngeal dysfunction), and either primary or metastatic neoplasia involving bronchi or the trachea. Idiopathic pulmonary fibrosis (with bronchial involvement) can be associated with cough in conjunction with tachypnea. This article focuses on respiratory causes of chronic cough in dogs.
History and Physical Examination
A thorough history is helpful for distinguishing among the differential diagnoses for the cough. Knowing the patient’s geographic location, travel history, and environment will help you form a list of differential diagnoses. This list can be refined by considering signalment and findings from the physical examination, including careful cervical and thoracic auscultation. Auscultation of soft pulmonary crackles, tachycardia, heart murmur, gallop sound, or arrhythmia suggests cardiac disease. Auscultation of loud pulmonary crackles, bradycardia, wheezes, or stridor suggests respiratory disease. The differential diagnoses for crackles include pneumonia, pulmonary edema, airway collapse, chronic bronchitis, or pulmonary fibrosis. Auscultation of wheezes suggests narrowed bronchi, which can occur in dogs with chronic bronchitis. Dull breath sounds can indicate pleural effusion, pneumothorax, intrathoracic mass, or diaphragmatic hernia (but they can also be heard in a patient with a thick body wall and/or deep chest).
Diagnosis
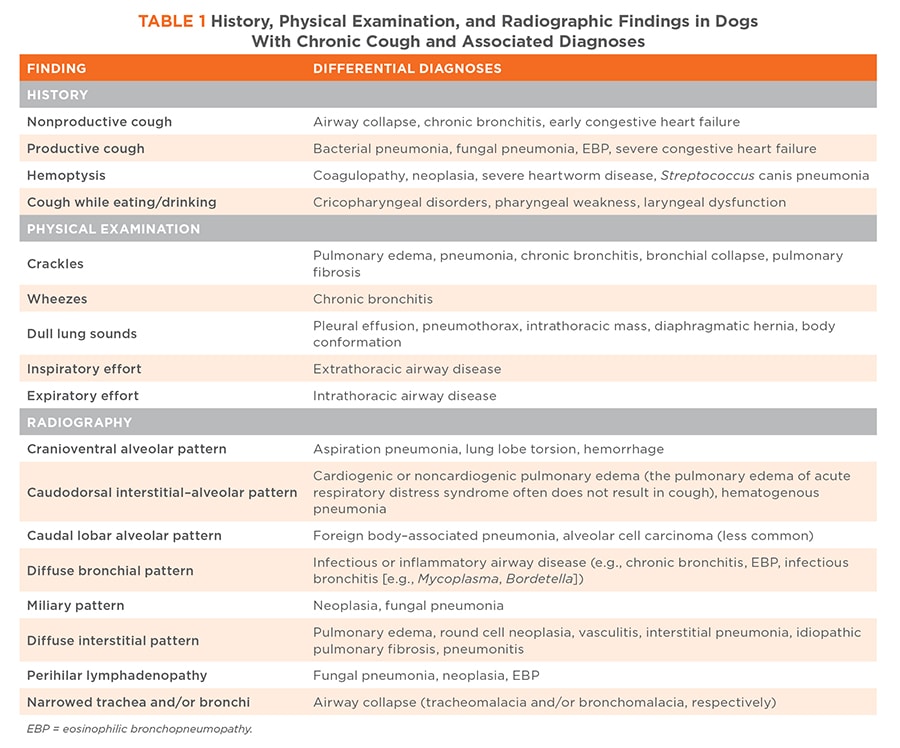
Consider various differential diagnoses before selecting diagnostic tests and planning appropriate treatment for chronic cough in a dog. The recommended minimum database includes complete blood count, heartworm antigen testing, and cervicothoracic radiographs. The most valuable initial diagnostic test for the chronically coughing patient is 3-view thoracic and lateral neck radiography (FIGURE 1). The radiographic pattern and distribution of pulmonary changes are often helpful for prioritizing differential diagnoses for these patients (TABLE 1).
Because of the dynamic nature of airway collapse, survey radiographs often lead to underdiagnosis of this condition. Therefore, to identify tracheal or bronchial collapse, video fluoroscopy or multiple radiographic images are often needed.1
Advanced respiratory diagnostics are sometimes necessary for obtaining a definitive diagnosis for chronic cough. Bronchoscopy with the patient under general anesthesia enables visualization of the airways and bronchoalveolar lavage for cytologic evaluation, bacterial culture and susceptibility testing, and polymerase chain reaction if indicated.2 If bronchoscopy is unavailable, transtracheal wash of a sedated patient or endotracheal wash with a sterile endotracheal tube and a sterile sampling airway catheter with the patient under light anesthesia can be readily performed in general practice (FIGURES 2 AND 3).
Treatment
If the history, physical examination, and diagnostics confirm that the cough is respiratory in origin, management should address the underlying cause; however, regardless of underlying cause, most patients benefit from various nonspecific strategies. The most useful strategy is weight loss for overweight dogs. Another strategy is airway nebulization with sterile saline 2 to 3 times per day, which will humidify and help clear airway mucus. To ensure that the sterile saline reaches the distal airways, use of an ultrasonic nebulizer that generates particles smaller than 5 microns is recommended. Nebulization can be followed with gentle exercise or thoracic coupage to promote expectoration. Oral N-acetylcysteine (125 to 600 mg PO q12h to q8h) can act as a mucolytic and improve mucus clearance in dogs with exudative and inspissated respiratory secretions; this drug also has antioxidant properties because it can increase endogenous glutathione levels.3 More specific treatments vary according to the underlying cause of the cough.
Bacterial Infections
For aspiration, infectious, or hematogenous bacterial pneumonia, administration of antibiotics for 2 to 4 weeks is typically necessary, depending on the severity and underlying comorbidities. Antibiotics with good pulmonary tissue penetration include azithromycin, doxycycline, clindamycin, trimethoprim-sulfamethoxazole, and fluoroquinolones (e.g., enrofloxacin and marbofloxacin). Antibiotic therapy should be combined with nebulization. Before antibiotics are discontinued, follow-up radiographs should be taken to document resolution of the bacterial pneumonia. Two bacteria that can cause an insidious chronic cough are Mycoplasma canis and Bordetella bronchiseptica; the antibiotic of choice for infection with these 2 organisms is doxycycline. TABLE 2 lists additional antibiotics appropriate for bacterial pneumonia.

Chronic Bronchitis
A common inflammatory airway disease of middle-aged dogs is chronic bronchitis. Apart from their chronic cough, patients with this condition are usually systemically healthy. Often, thoracic radiographs show a bronchial pattern. Chronic bronchitis is a diagnosis of exclusion and is confirmed by finding nondegenerate, nonseptic, neutrophilic inflammation in airway samples.2 In addition to the above nonspecific recommendations for coughing (i.e., mucolytics and humidification), the treatment of choice for dogs with chronic bronchitis is anti-inflammatories with oral glucocorticoids initially and inhaled glucocorticoids chronically (FIGURE 4). To minimize the systemic side effects of oral glucocorticoids, fluticasone (110 mcg/puff in a metered dose inhaler) can be administered twice daily via an aerosol chamber and adapter. The dog can be slowly acclimated to this device before the steroid inhaler is introduced. An advantage of this treatment is that it can be continued for a long duration; a disadvantage is the fluticasone expense.
Eosinophilic Bronchopneumopathy
EBP is another inflammatory lung disease that occurs in young to middle-aged dogs; predisposed breeds are huskies and Rottweilers. Approximately 50% of these dogs will have chronic nasal discharge and sneezing, and 50% will have peripheral eosinophilia. In contrast to chronic neutrophilic bronchitis, dogs with EBP often are systemically unwell and thoracic radiographs can show an alveolar component in addition to a bronchial pattern. Before a diagnosis of EBP is reached, other causes of eosinophilic airway inflammation must be ruled out (including heartworm disease via serology and lung worms via fecal testing). Treatment is similar to that for chronic bronchitis, except that for many of these dogs more aggressive and possibly long-term glucocorticoid treatment is needed. For some dogs, oral modified cyclosporine (5 mg/kg PO q12h) might also be considered. Inhaled glucocorticoids are often used, although some dogs are refractory to this therapy.4
Airway Collapse
Management of airway collapse is multifactorial and includes avoiding stressful situations and using a harness instead of a neck leash for handling these dogs. Weight loss can be the most valuable management component but also the most challenging to achieve because of lack of client compliance and the dog’s inability to exercise because of its airway disease.1 For the medical component of treatment, theophylline can be helpful. Although theophylline is a weak bronchodilator, it improves mucociliary clearance and has immunomodulatory properties. It can also help improve expiratory airflow, thus helping to reduce the tendency for airways to collapse. Some dogs with chronic bronchitis and airway collapse can benefit from oral or inhaled glucocorticoid therapy. When causes of cough other than airway collapse have been ruled out, cough suppression with antitussive drugs such as hydrocodone (0.22 mg/kg PO q6 to 12h) is often necessary, particularly when the dog is stressed or excited. A salvage procedure for end-stage tracheal collapse is placement of a nickel-titanium alloy tracheal stent; this procedure is more often recommended for dogs with difficulty breathing rather than those with chronic cough. For these dogs, thorough bronchoscopy is paramount for ruling out comorbidities such as bronchial collapse or chronic bronchitis because if significant cough persists after stent placement, the stent is at greater risk of fracture or migration.
Fungal Infections
Fungal pneumonias are suggested by geography and travel history, weight loss, fever, miliary pattern with hilar lymphadenopathy on thoracic radiographs, hyperglobulinemia, and a chronic progressive course of illness. Diagnosis is based on a combination of these findings along with results from either serologic (for coccidioidomycosis and cryptococcosis) or urine antigen (for aspergillosis, blastomycosis, and histoplasmosis) testing.5 Also diagnostic is fine-needle aspirate cytology of lymph nodes, skin lesions, or pulmonary nodules. Treatment depends on the underlying organism but typically consists of a minimum of 6 months of oral azole therapy and, depending on the case, initial IV administration of either amphotericin B lipid complex or an echinocandin.6
Foreign Bodies
Airway foreign bodies tend to cause an acute cough, generally in active large breed dogs, but can cause chronic signs if undiagnosed. The index of suspicion for an inhaled foreign body is raised when focal chronic consolidation of the caudal lung lobe is seen on thoracic radiographs after the patient has received antibiotics for 1 to 2 weeks. Foreign bodies should ideally be removed with bronchoscopic assistance before they migrate out of the airways and into the parenchyma, pleural space, or peritoneum. Chronic airway foreign bodies can also be associated with lung abscessation or pyothorax, which might require thoracotomy and lung lobectomy.
Dysphagia
Dysphagia with or without laryngeal dysfunction can cause a chronic cough.7 Some dogs with dysphagia will show signs of nasal disease resulting from aspiration of food or water into the nasopharynx. The age distribution for dogs with dysphagia is often bimodal: young dogs may have developmental diseases (e.g., cricopharyngeal achalasia/asynchrony, megaesophagus, or brachycephalic syndrome), and old dogs may have degenerative neurologic disorders (e.g., geriatric-onset laryngeal paralysis polyneuropathy).8 All dysphagic dogs are susceptible to aspiration pneumonitis and/or pneumonia. They require specific management of esophageal and airway dysfunction when possible (e.g., upright feeding, altered food consistency, and judicious use of acid suppressants). For dogs with brachycephalic syndrome, early surgical correction of obstructive airway lesions is advised.
Neoplasia
Chronic cough in middle-aged to older dogs can indicate primary or metastatic pulmonary neoplasia, which is often visible on survey radiographs.9 Thoracic radiographs can show pulmonary nodules >5 mm, and contrast computed tomography can show pulmonary nodules as small as 2 mm.9 Primary lung neoplasia can be addressed with surgery or chemotherapy; metastatic pulmonary neoplasia can be addressed with palliative treatment and chemotherapy.
Summary
In summary, chronic cough is a common presenting complaint for dogs of all ages. After cardiac causes of cough are ruled out, the differential list of respiratory causes can be narrowed down by using signalment, history, physical examination, CBC, and survey cervicothoracic radiographs. When the cause of cough is not apparent based on these diagnostics and persists despite empiric treatment, then referral to an internal medicine specialist for further diagnostics, including airway sampling, is recommended.