Epilepsy in dogs is a common disease—thought to affect up to 1 in 20 dogs—and potentially life threatening.1 A useful working understanding is essential for the small animal practitioner.
Editor’s Note: This article was originally published in 2014. Please use this content for reference or educational purposes, but note that it is not being actively vetted after publication. For the most recent peer-reviewed content, see our issue archive.
When a patient presents for an episode of odd behavior or movement, the clinician must immediately consider 4 questions:
- Are the events described by the owner (or recorded on video) truly a seizure?
- Can an underlying cause be identified and treated versus treating only the seizure?
- Should an anti-epileptic drug (AED) be administered?
- If medical therapy is pursued, which AED should be chosen?
1. IS THE EVENT A SEIZURE?
There are many behaviors, events, and diseases that mimic a true seizure (Table 1).
Electroencephalography
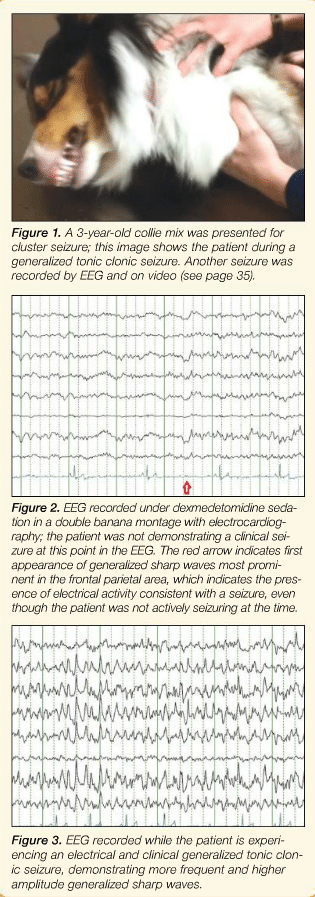
Electroencephalography (EEG) records the brain’s electrical activity and is considered by many human physicians to be an essential tool for characterizing seizure events (Figures 1-3). However, EEG is not a readily available clinical tool in veterinary medicine, and a first-time EEG recorded between seizures in an epileptic human or dog has about a 25% chance of identifying the event as a seizure.7
Observation
Identification of a seizure is most often achieved by comparing the observed event to what is considered a typical seizure.
- Generalized tonic clonic seizures typically last 1 to 2 minutes, and characteristically feature loss of consciousness, muscle tone and movement (tonic/clonic), jaw chomping, and profuse salivation, followed by gradual return to consciousness and normal ambulation.
- Partial or nonconvulsive seizures are more difficult to recognize, with the latter requiring an EEG recording during the event.8
In human medicine, classifying events by description alone (without EEG) is accurate, but also allows overdiagnosis of nonepileptic events as seizures. Therefore, observation has high sensitivity, low specificity, and low positive predictive value.9 Accordingly, clinicians should be aware that they may be treating nonepileptic events with an AED.10
2. DOES THE SEIZURE HAVE AN UNDERLYING CAUSE?
Identifying an underlying cause for the seizure yields better seizure control, quality of life, and accurate prognosis. The most recent seizure classification system—by cause—groups seizures into 3 causes: genetic, structural/metabolic, and unknown.
Genetic & Unknown Causes
Diagnosis of idiopathic epilepsy (IE) is made when:
- Genetic basis is suspected
- Testing has failed to reveal a cause for the seizure.
Structural/Metabolic Causes
- Diagnosis of structural epilepsy is often made by magnetic resonance imaging (MRI) and cerebrospinal fluid (CSF) analysis, with common causes, including brain tumor, infarct or hemorrhage, or encephalitis.
- Technically, most metabolic causes of seizure are not a form of epilepsy because the brain itself is normal and reacting to an extracranial insult, which once eliminated, results in cessation of seizure.
Because MRI and CSF analysis are expensive and not readily available, the primary care clinician is often faced with making a difficult decision about whether to refer a patient or simply prescribe an AED. Key factors in assessing a seizure patient include:
Age
As a guideline, dogs with IE typically have their first seizure between 6 months and 6 years of age. However, at seizure onset, about 20% of dogs older than 6 years, and 2% of dogs younger than 6 months, do not have an identifiable cause for seizure.11
Breed
There are, however, some exceptions to the age rule noted above. Seizure is a very common presenting complaint in dogs with brain tumors such that, in certain breeds (eg, golden retriever, boxer, Boston terrier, French bulldog), even 1 seizure at 4 years or older should be cause for concern.12 In young (1-5 years of age), small breed dogs (eg, pug, Chihuahua, Maltese, poodle) that have 3 or more seizures within a few months, meningoencephalitis of unknown etiology (MUE) should be considered a likely cause for the seizures.
Behavior
Even subtle behavior changes around the time of the first seizure indicate that a patient is likely to have symptomatic epilepsy (Table 2).
Examination Findings
If a neurologic examination performed between seizures has abnormal results, there is a high probability that a structural brain lesion is the cause of the seizure. However, 30% of brain tumor patients will have a normal examination, and 18% of idiopathic epileptics can have a transiently abnormal examination.10
It is useful to observe a seizure patient in the examination room to evaluate gait and behavior, coupled with an examination of the postural reactions and menace response. As a guideline, the following findings suggest structural disease, although other causes are possible:
- Confusion
- Circling to one side
- Postural reaction
- Menace deficits on one side.
3. SHOULD AN AED BE ADMINISTERED?
AED drug therapy is recommended if any of the following are present/occur:
- Structural cause for the seizure
- Severe first seizure or post-ictal period
- Owner preference to reduce chances of another seizure.
For IE, I recommend AED therapy after 1 or 2 seizures in a 6- to 12-month period for several reasons:
- Although rarely life-threatening, seizures are very upsetting to owners, and a recent owner survey showed that most owners felt the only acceptable seizure control is no seizure.13
- AED therapy likely reduces the chance of a life-threatening seizure/status epilepticus.
- Although controversial, there is both bench-top and clinical data that demonstrates every seizure a patient experiences increases the chance for another seizure, independent of the seizure cause. In other words, seizure begets seizure.14,15
- Newer generation AEDs do not have as many side effects or organ toxicities compared to older AEDs, and are now available in generic or cost-effective formulations (Table 3).16-18
4. WHICH AED SHOULD BE CHOSEN FOR THERAPY?
Maintenance Therapy
When and which AED to apply in the clinical setting remains uncertain and controversial (see Studies Evaluating AED Efficacy & Safety). Some reasonable guidelines for seizure management are to:
- Use one medication at a time
- Choose medications with best efficacy, lowest cost/dosing interval, fewest side effects, and lowest risk of toxicity.
Table 3 lists AEDs in the order they are used by most neurologists in our clinic.11,19
When to Change. Side effects or lack of efficacy can prompt the need to change AEDs. Studies show that only about 70% of dogs are well controlled on an AED,17 and fewer than half the dogs on phenobarbital and/or bromide are seizure-free without adverse medication-related side effects.20
Treating with multiple AEDs may be beneficial because they act on a broader range of mechanisms or synergistically; however, side effects can be additive, and determining which AED is effective is difficult when more than one medication is administered. Generally, I recommend using one AED at a time; therefore, AEDs often need to be switched rather than added.
Transition Period. Abrupt cessation or missed doses of AEDs is a common cause of seizure and status epilepticus in humans. This may be of less concern in dogs—only 6% of status epilepticus cases in one study resulted from low AED concentration.26 Nevertheless, tapering the dose prior to stopping an AED is recommended. Risk of seizure can be further reduced if at least one AED is maintained in the therapeutic range during the transition. See Step-by-Step: Transitioning to Newer Generation AEDs.
Rescue Therapy
AED therapy—additional or different, oral or parenteral—to control cluster seizures or status epilepticus is called rescue therapy. Rescue plans for epilepsy patients are recommended because, among dogs being treated for IE, a 59% incidence of status epilepticus and higher rates of cluster seizures have been described.27 Furthermore, a 25% mortality rate among all dogs that present for status epilepticus has been reported.26
Predicting Seizures. Recent EEG evidence suggests seizures in dogs are not random events, and that forecasting seizures is possible.28 Therefore, while therapy can be initiated after a seizure, it can potentially be administered before a seizure, as many owners feel they can predict when seizures will occur.
Oral Therapy. Oral rescue therapy is appropriate if time to next seizure is an hour or greater, allowing for gastrointestinal absorption and development of useful serum concentration. For example, levetiracetam takes about 81 minutes to reach maximal serum concentration following oral administration.29
Although studies are lacking, administration of an extra dose of maintenance AED and initiation of a novel AED for a short period of time (pulse therapy) is advised to control cluster seizures and status epilepticus (Table 4).
I advise owners to give a dose of AED used for pulse therapy between seizures to assess side effects, and determine best tolerated dose, prior to using the medication in the post-ictal period.
Other Types of Therapy. Intranasal (IN), subcutaneous (SC), intramuscular (IM), and rectal AED administration have been advocated when (Table 5):
- Patient is unable to swallow
- Rapid cessation of seizure activity is required
- Intravenous (IV) route is unavailable.
I advise owners to give levetiracetam (60 mg/kg SC) plus midazolam (0.2 mg/kg IM) or diazepam injectable solution (2 mg/kg by rectum).
AED = anti-epileptic drug; CSF = cerebrospinal fluid; EEG = electroencephalography; IE = idiopathic epilepsy; IM = intramuscular; IN = Intranasal; IV = intravenous; MRI = magnetic resonance imaging; MUE = meningoencephalitis of unknown etiology; SC = subcutaneous